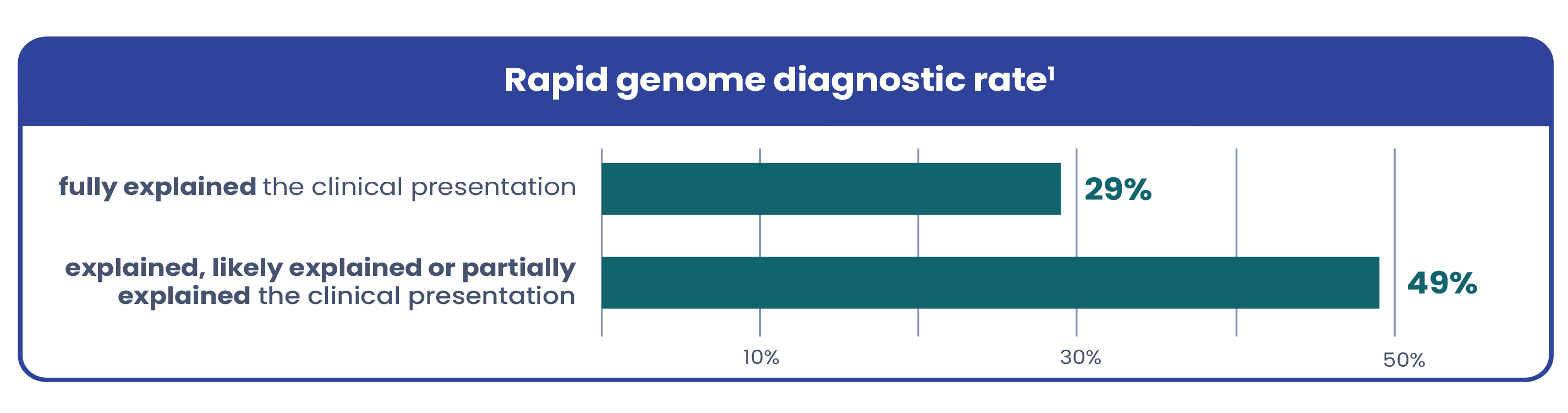
fully explained the clinical presentation
29%
explained, likely explained or partially explained the clinical presentation
10%
30%
50%
50%
49%
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Suspendisse varius enim in eros elementum tristique. Duis cursus, mi quis viverra ornare, eros dolor interdum nulla, ut commodo diam libero vitae erat. Aenean faucibus nibh et justo cursus id rutrum lorem imperdiet. Nunc ut sem vitae risus tristique posuere.

Of infants admitted to level IV NICUs admissions are likely eligible for rapid genome sequencing1.
Of eligible patients receive rapid testing2. For these critically ill infants, every moment matters. Rapid genome sequencing can provide an early and precise diagnosis–enabling timely interventions, reducing hospital stays, and improving outcomes3,4.
Due to variable and complex presentations, genetic conditions in critically ill infants are often hard to recognize based on symptoms alone. Current testing workflows are often too narrow, leaving many patients undiagnosed. A recent study in The American Journal of Human Genetics found that among the infants who received a genetic diagnosis via rapid genome with a broad testing protocol1:
Testing all infants whose clinical condition is not fully explained by trauma, infection, or prematurity leads to more diagnoses and maintains a high diagnostic yield1.
Implementing rapid genome sequencing as a first-line test in NICU workflows is proven to:

Change medical management for up to 87% of babies.
Reduce healthcare costs up to $15,786 per child.
Learn more about whole genome sequencing and whole exome sequencing.


Infinity is shaped by the data of real people and real cases – and it’s changing what’s possible in rare disease care. It helps us see more clearly, diagnose more confidently, and discover insights that lead to better answers for more families.
Layla was born with a bowel obstruction that required two emergency surgeries in her first weeks of life. Considered as a typical short-bowel patient, Layla didn’t respond to treatment as expected. Fortunately, her care team used GeneDx rapid genome sequencing to uncover TTC7A deficiency, a rare condition that affects both the intestines and the immune system. Learn how her treatment drastically changed—helping Layla not just survive, but thrive.

GeneDx provides one reanalysis at no additional charge per genome order, recommended at least one year after the original analysis to maximize gene discovery and to identify new patient phenotypes that may inform reporting (especially in the NICU population).
Infinity is powered by data from over 2.5 million tests – informed by nearly 1 million exomes and genomes and more than 7 million phenotypic datapoints – to help you uncover answers faster and fuel the discovery of life-changing treatments.
Access the Rapid Genome Ordering Guide for NICU teams—featuring step-by-step ordering instructions, specimen guidance, and contact pathways for the dedicated Xpress support team.
We’re here to support every step.